Well ladies and gentlemen, it’s hard out there for an avenger. Take this first case – this is actually the unfortunate child of one of my arch enemies. The last time we fought, I hit him so hard, his kid developed ectopia lentis.
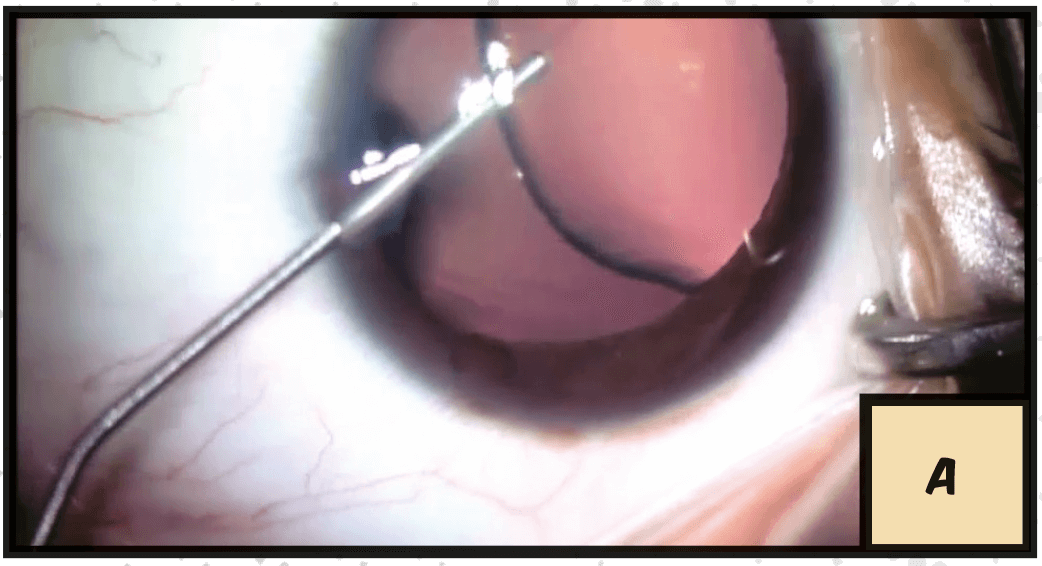
A. As you can see here we’ve got a very dislocated lens, about 50 percent visible through the pupillary aperture, so we put in viscoelastic to block any vitreous from coming through those weakened zonules.
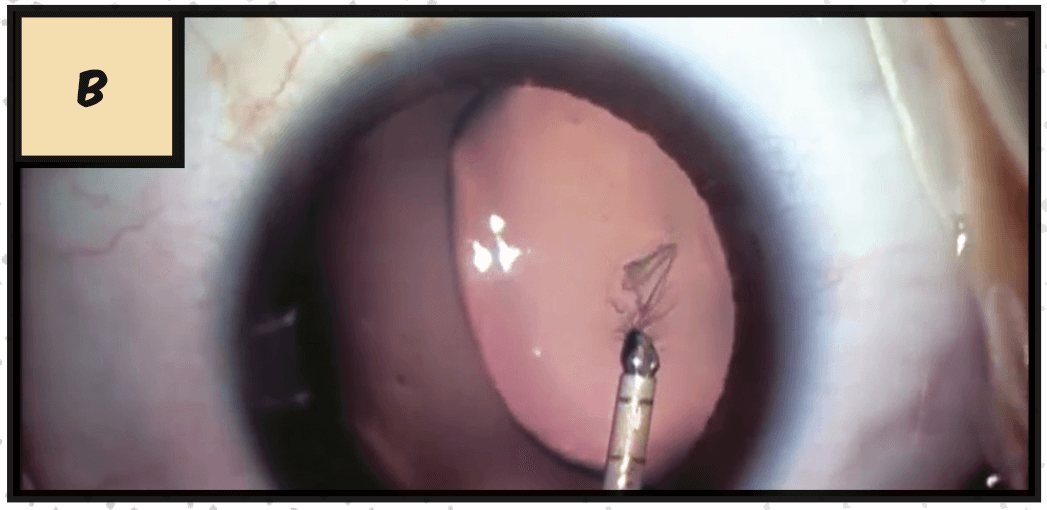
B. Now we start our rhexis here with a cystotome, and then we’re going to use some forceps – a pediatric capsule is very elastic, so I like a micro capsulorhexis forceps.
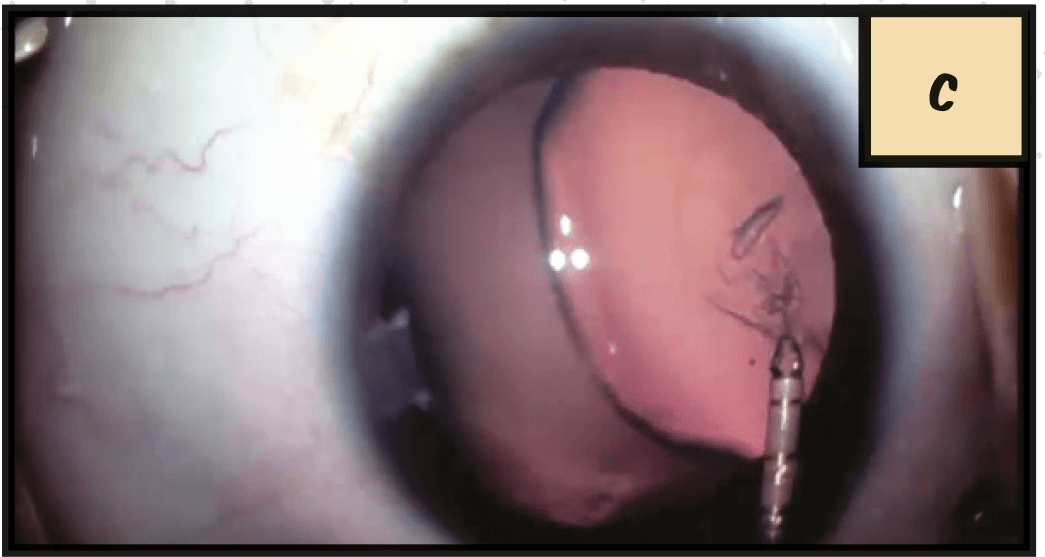
C. We’re going through the main incision here as I’m able to do most of the work through this, but I can also go through a paracentesis if I need to. I’m pulling against the direction of the tear, so that the ‘rhexis doesn’t go out, and I can get a good size.
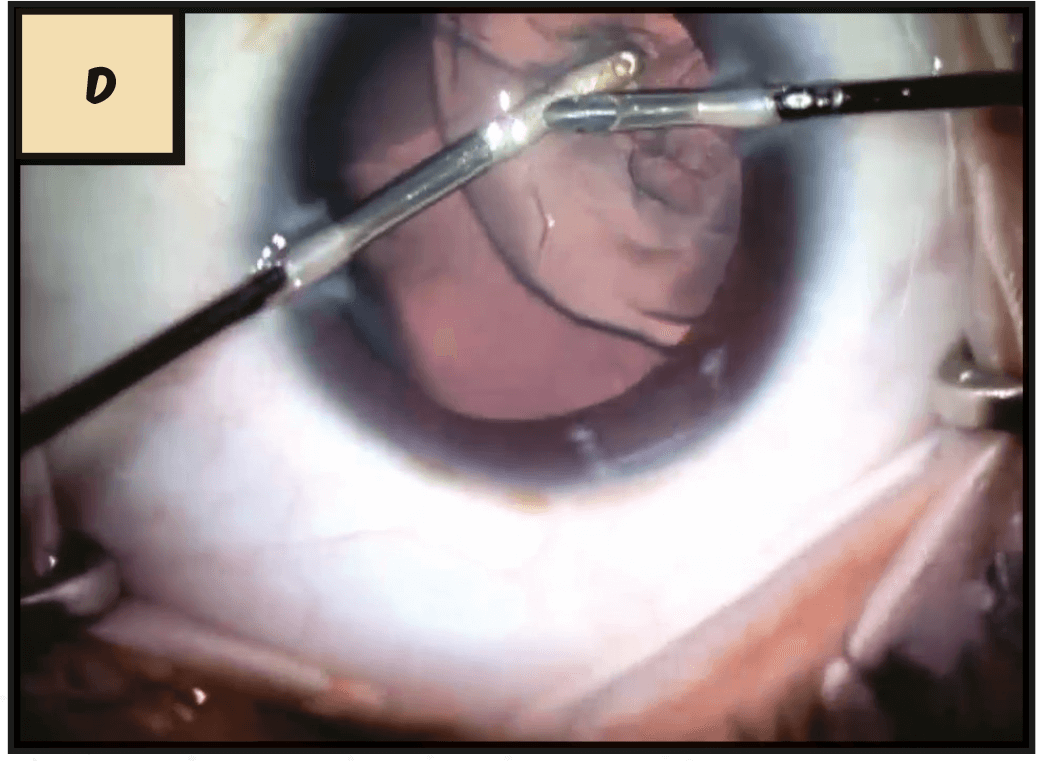
D. Remember, you don’t need a very big ‘rhexis in a kid’s eye; a small one will suffice. We’ll do a thorough hydrodissection, and I replace my viscoelastic to make sure I’ve got good vitreous tamponade, and I just use I&A to take these lenses out, as they’re very soft.
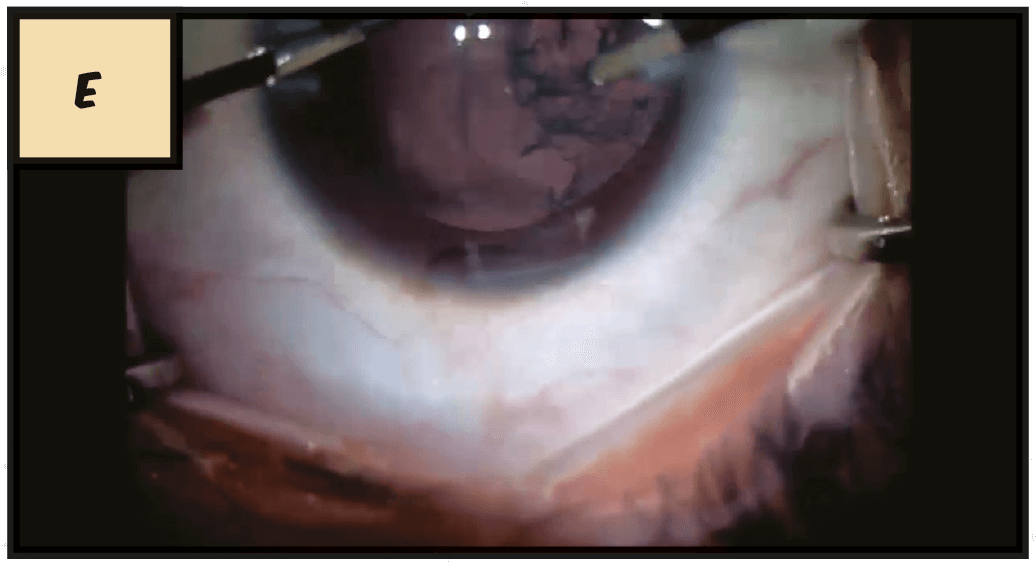
E. In a non-dislocated lens, I’ll use a coaxial I&A, because I’ve got the big port, but with this case I use bimanual, so I can come from either side. Now I wasn’t able to get it all easily, so I fill with viscoelastic and try to put my CTR in. I also do a little viscodissection to get any cortex off the anterior capsule.
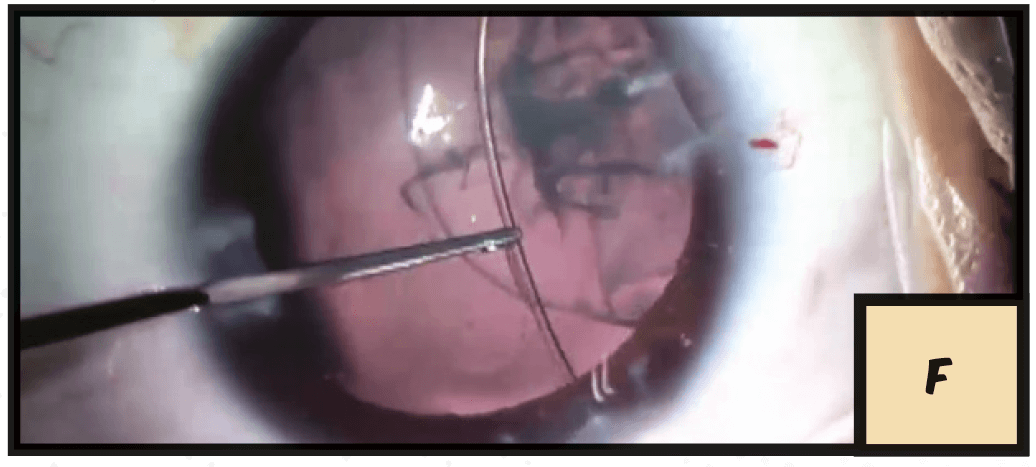
F. Now we like to dial our ring in from the strong area into the weak area, but that would be difficult in this direction. And even in the other direction I can’t make it happen, so I’m going to take my ring out and not force it.
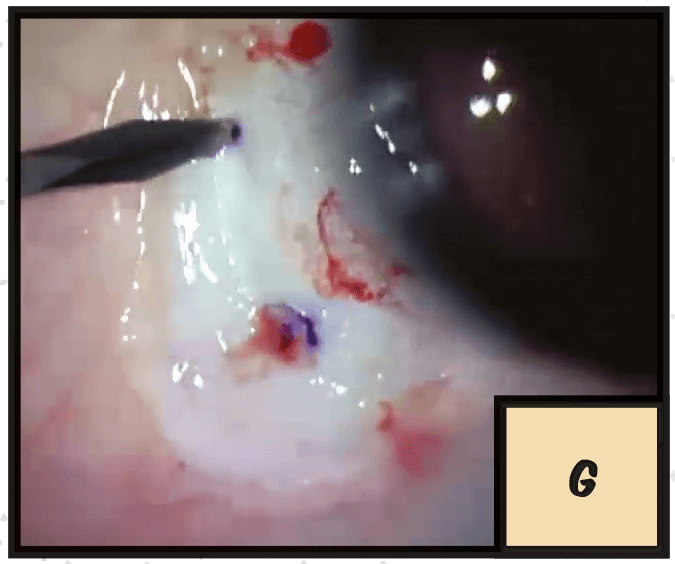
G. And getting a little bit more of that ring going in actually loosened my cortex, so I can get most of it. I make a little peritomy, and I just like to do two side port incisions here, about 2 mm from the limbus.
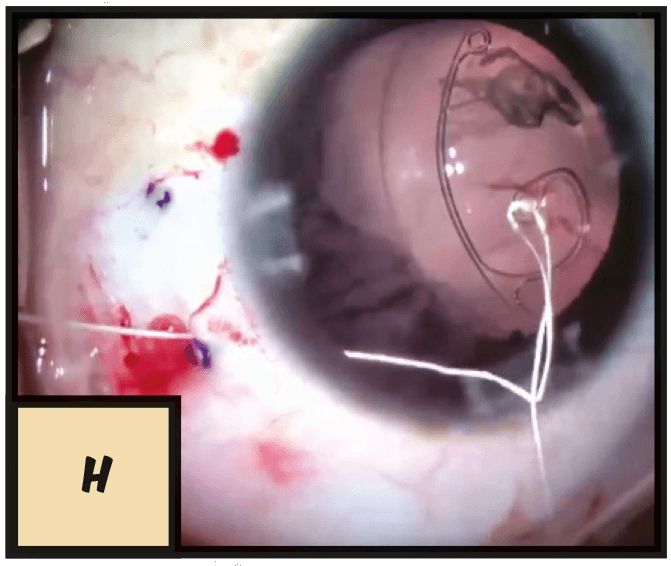
H. When you have an intact vitreous they don’t leak, so they work very easily. I’m going to put in an Ahmed segment here, and I like to use a Gore-Tex suture. This is a kid, so this is going to be in their eye for a very long time. If I use a Prolene suture, I know it’s going to degrade eventually, and I’m going to have to replace that, or fix a dislocated lens.
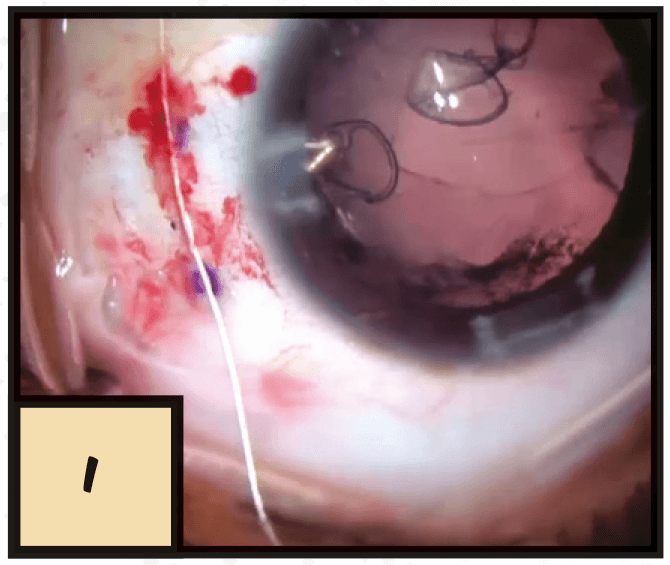
I. I put a little groove in between those incisions so that suture sits down really nicely, and then I can pull my capsule over.
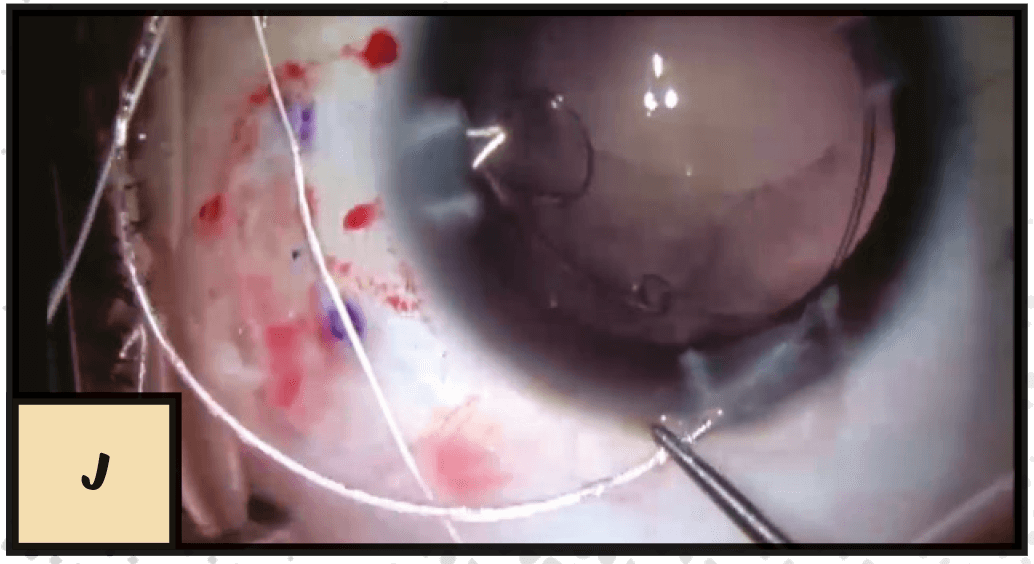
J. Now I can finish my viscoelastic removal, and dial the ring in. I like doing this with instruments rather than an injector, I think I can feel it a little bit better. I drop that ring in with a Sinskey, then I can suture that and finally place my capsule. When you do the capsular tension segment in without the ring, it can tilt, so you don’t want to pull it too tight, or you can actually pull it out of the capsule.
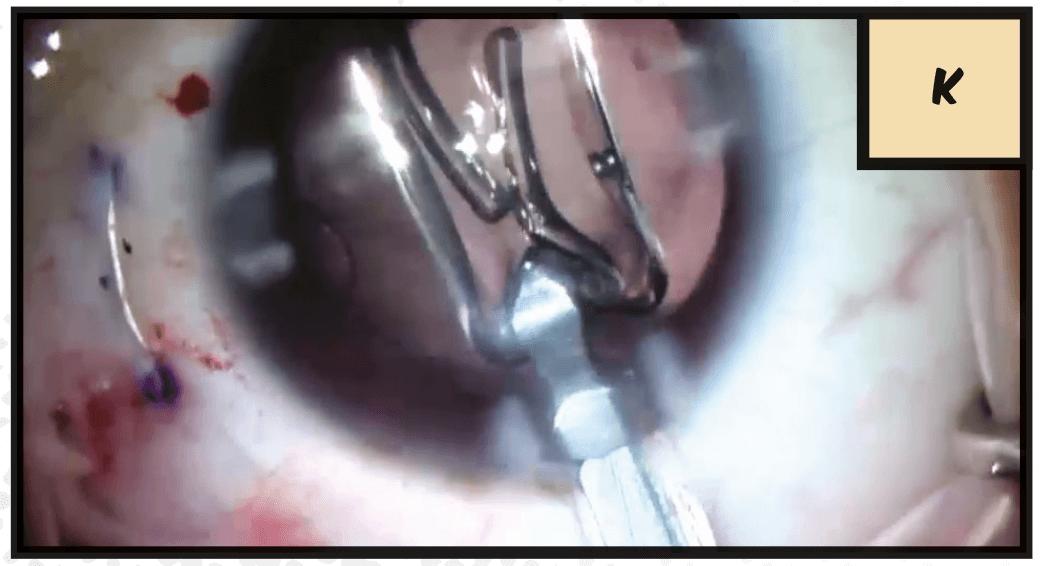
K. Now I can inject my lens very easily, and I’ve got a case with a lens in the bag, in a kid who has a good future ahead of him.