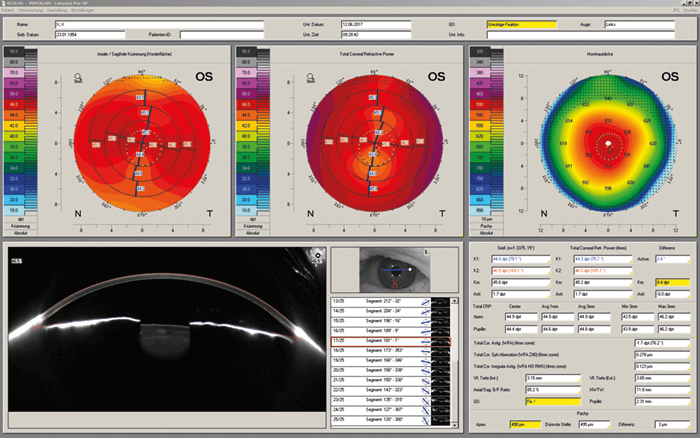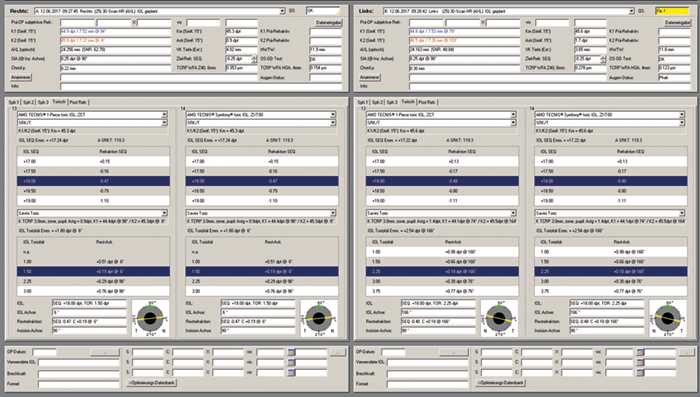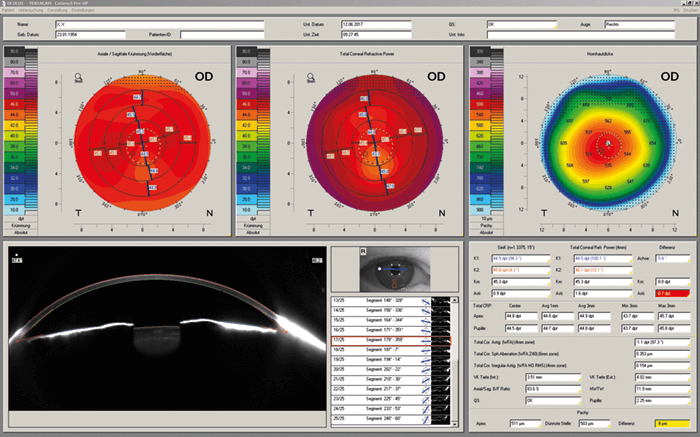
All surgeons want the best for their patients, and when it comes to refractive outcomes, anterior segment analysis plays a key role. The Pentacam® and Pentacam® HR provide a gold-standard in anterior segment tomography. Now meet the newest member of the family – the Pentacam® AXL. Based on the trusted Pentacam® HR system, which offers high-resolution Scheimpflug imaging, the Pentacam® AXL offers the additional feature of axial length measurement – a crucial part of accurate IOL calculation and customized IOL selection. Through partial coherence interferometry biometry, the Pentacam® AXL collects several successive axial length measurements; patient eye movement is detected by the pupil camera and corrected for, and a 3D model of the anterior segment based on ray tracing allows for the correction of individual optical distortions. Using fourth generation IOL formulas, the system can automatically calculate IOL power. Because the total corneal refractive power (TCRP) map shows the influence of the posterior corneal surface with regard to total corneal astigmatism axis, magnitude and regularity, the IOL calculation software can account for posterior corneal astigmatism. The software also accounts for prior refractive surgery and pre-existing conditions, ensuring a reliable IOL power calculation for any IOL type in both virgin and post-refractive eyes. The upshot? The Pentacam® AXL enables full screening before corneal refractive and cataract procedures. Laser vision correction procedures can be planned effectively; patients can be screened for existing diseases such as Fuchs endothelial dystrophy or angle-closure glaucoma; prior refractive surgeries can be detected; and crystal lens densitometry can be used to plan femtosecond laser-assisted cataract surgery (FLACS). Now, accurate IOL calculation can also be achieved – as well as customized IOL selection regarding multifocal, toric and aspheric IOLs, all from one device.